
Health economics has been a field of economics that draws great interest since the publication of Kenneth J. Arrow’s article Uncertainty and the Welfare Economics of Medical Care in 1963. In neoclassical economics, human capital is perceived to be one of the major determinants of long-term economic growth. Education and health care play a key role in the formation of human capital. Without healthy labour the production process is severely obstructed. The degradation of the general health has also negative implications for the society that go beyond the marketplace. Better health is central to human happiness and well-being. It also makes an imperative contribution to economic progress, as healthy populations live longer, are more productive, and save more.
Current State of Health Care in Egypt
It is no secret that Egypt has a failing and unequal public health service, which does not adequately respond to the demands of majority of citizens. The health care service is not only underfunded but also understaffed. Egypt lacks well-trained nursing staff and doctors in addition to the poor state of public hospitals.. According to the World Bank, in 2012 Egypt has 0.5 hospital beds per 1000 people, whereas a country like Brazil has 2.3, China 3.8, Israel 3.3 and 1.5 for Mexico. More advanced economies such as Germany have 8.2 hospital beds per 1000 people. The Egyptian Ministry of Health statistics show that the number of government hospitals in 2011 was 643 with 98, 319 beds, 19 general hospitals, 38 health insurance authority hospitals and 74 public university hospitals whereas the number of private hospitals was 926 with 25,827. Although the amount spent on health care has increased in monetary terms over the past decade, the share of healthcare spending as a percentage of GDP has been decreasing over time as can be seen from figure 1.
Figure 1: Health Sector Share of GDP at Factor Cost
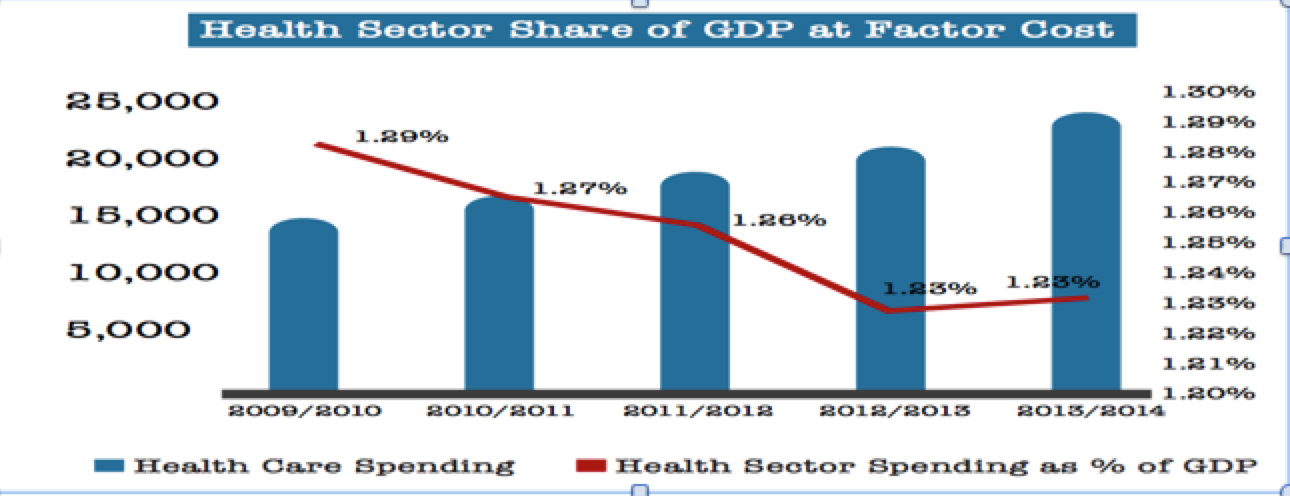
Source: Multiples Group – Health Care Sector Report, Egypt 2015
Non-communicable diseases such as cancers, diabetes, obesity and chronic respiratory diseases have become more widespread in recent years in Egypt than communicable diseases as illustrated in figure 2. Non-communicable diseases are not only more rampant but also more costly to treat. The incidence of diabetes has risen considerably in recent years. Presently, estimates of 16.5 million people in Egypt are diabetic, ranking it 9th in the world.
Figure 2: Prevalent Diseases in Egypt
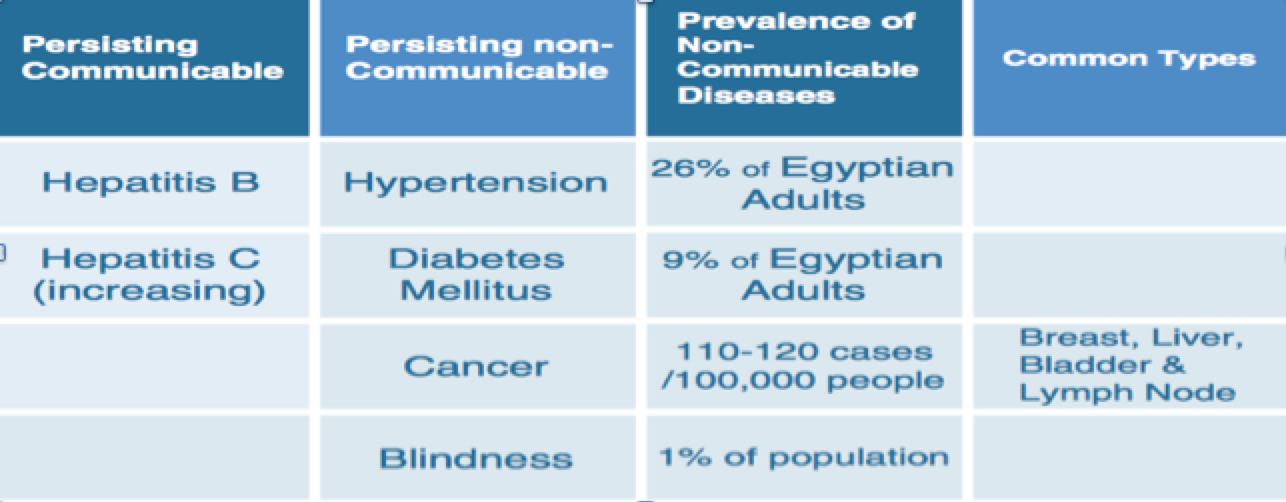
Source: WHO 2013
Furthermore, as figure 3 illustrates, the amount spent on health care as a percentage of total government expenditure remains far below the averages of international governments.
Figure 3: Egypt Vs World Average

Source: Central Bank of Egypt
Better Health Outcomes are Attainable despite Budget Constraints
Some argue that Egypt cannot afford to increase its health expenditure due to budget constraints. Egypt has been undergoing a tight austerity programme since Abd- El Fattah El Sisi came to power in order to reduce the widening budget deficit and bring public debt to safe levels. The first ignored element by the proponents of the argument that Egypt is a poor country and cannot offer to increase health care expenditure and quality is the fact that basic level healthcare is a very labour-intensive activity, and in a poor country wages are low. A poor country like Egypt may have less money to spend on healthcare, but it also needs to spend less to provide the same labour-intensive services (far less than what a richer – and higher-wage – economy would have to pay).
Furthermore, Nobel Prize winner Amartya Sen states “how much healthcare can be provided to all may well depend on the country’s economic ability, but whatever is affordable within a country’s means can still be more effectively and more equitably delivered via universal coverage”. Given the hugely unequal distribution of incomes in an economy such as Egypt, there can be serious inefficiency as well as unfairness in leaving the distribution of healthcare entirely to people’s respective abilities to buy medical services.
Public Vs Private
Many medical and health services are shared, rather than being exclusively used by each individual separately. An epidemiological intervention, for instance, spreads to many people who live in the same neighbourhood, rather than only one person at a time. Healthcare, thus, has strong components of what in economics is called a “collective good” or a “public good”, which typically is very inefficiently allocated by the pure market system and requires extensive intervention by the state for its provision. According to mainstream economic theory, leaving a public good for private provision will induce private agents to produce less of the good at a high price. Private agents will not provide health service for free since the majority will tend to free ride (market failure).
In the absence of a reasonably well-organised system of public healthcare for all, many people are distressed by overpriced and inefficient private healthcare. There cannot be a well-informed competitive market equilibrium in the field of health care, because of what is known as “asymmetric information” in the economics profession. Patients normally have very limited knowledge about the product – health care, therefore, they tend to heavily rely on their physicians to give medical advises. Patients do not normally know what treatment they need for their illness, or what medicine would function for their ailments, or even what exactly the doctor is giving to them as a remedy. The problem of asymmetric information applies to the delivery of medical services itself. It makes the possibility of exploitation of the relatively ignorant a likely result even when there is plentiful market competition.
Thus, in advanced economies there is a widespread of not-for-profit providers in the health care market. As mentioned earlier, this phenomenon is also explained by the fact that the information about health care is so unevenly distributed between patient and physician, so trust plays an important role in health care market transactions. Non-for-profit providers are viewed as more trustable because people tend to believe that profit motives would cause providers to abuse the information they have and induce patients to purchase health cares that are not necessary. As highlighted earlier, private hospitals in Egypt outnumber the failing public hospitals and consequently many Egyptian patients suffer from an overpriced and inefficient service. Even in public hospitals we observe in many incidents out of pocket expenditures in the form of bribery or forcing patients to purchase medications or medical equipment. A study conducted by Multiples Group (2015) shows that out of pocket expenditures as a percentage of total health expenditure in Egypt reach nearly 72% in comparison with only 35% in Turkey and 25% in Germany. This demonstrates the scope of the financial burden on poor Egyptian families who seek medical attention.
Success Stories from Developing Countries: Thailand
Thailand’s experience in universal healthcare is a good model, both in advancing health achievements across the board and in decreasing class and spatial inequalities. Similar to Egypt, Thailand has both a large population of 70 million people and per capita income of 5,200 dollars, whereas Egypt has an income per capita of 5,547 dollars according to UNDP data in 2015. Before the introduction of universal health care in 2001, there was a fairly good insurance coverage for about a quarter of the Thai population. This fortunate group comprised well-placed government servants, who qualified for a civil service medical benefit scheme, and employees in the privately owned organised sector, which had a mandatory social security scheme from 1990 onwards, and received some government subsidy. The bulk of the population had to continue to rely largely on out-of-pocket payments for medical care. Though, in 2001 the government introduced a “30 baht universal coverage programme” that, for the first time, covered all the population, with a guarantee that a patient would not have to pay more than 30 baht (about 60p) per visit for medical care (there is exemption for all charges for the poorer sections – about a quarter – of the population).
Amartya Sen in his Guardian article concludes that the result of universal health coverage in Thailand has been a significant fall in mortality (particularly infant and child mortality, with infant mortality as low as 11 per 1,000) and a remarkable rise in life expectancy, which is now more than 74 years at birth – major achievements for a poor country. There has also been an astonishing removal of historic inequalities in infant mortality between the impoverished and wealthier regions of Thailand; so much so that Thailand’s low infant mortality rate is now shared by the poorer and richer parts of the country. Other countries such as Costa Rica, Brazil, Cuba and the state of Kerala in India all provide good examples of low-income countries that have achieved improved health outcomes without draining the public budget. Better health outcomes through extensive investment in public health care has the potential to generate positive externalities for the rest of the society and may well enhance labors productivity in the long-run.
